
So far there’s not a lot on regional techniques or nerve blocks lurking around the site. Seems like we should change that. Dr Andrew Weatherall with a little bit about a super easy and super useful option – the fascia iliaca block.
At a time when opioids are slowly letting the happy veil slip we might be just about to usher in a golden age of blocks. Golden needles. Golden drugs. Golden sense of superiority in your dealings with that foul gorgon known as pain.
The advantages of regional techniques, or for today’s post peripheral nerve blockade are pretty numerous. Less use of other strong analgesics is certainly one of those benefits. A better quality of analgesia is likely to be on offer. Plus even when you know how they work, local anaesthetics are pretty impressive in action.
They do, sometimes, have a dark side associated with them too. Chief amongst these would be the risk of injury to nerve and the risk of injury to everyone involved (obviously mostly the patient but also staff) if the patient develops central nervous or cardiovascular toxicity.
It might be this or it might be an issue of timing and culture that probably inhibit people from getting on with a good block. And that’s not just a phenomenon for the operating theatre. There are plenty of clinical situations where the nerve block should really be undertaken in the emergency department. Or even before the emergency department.
Which brings us to the hero of this story – the fascia iliaca block.
The Story Begins
What were you doing in 1989? Wait, obviously only answer that if you were alive in 1989. If you weren’t alive yet, please show the old people grappling with their constant feeling of existential angst some space.
I remember bits of 1989 quite well. This is not because I made a point of memorising things that happened that year just in case future people invented a widespread knowledge and communication window system for recounting such stories. It’s because I got to visit France for a bit and tried out snails for the first time. To eat, not to wear or anything weird.
Around that same time when I was trying to figure out better solutions for what the Venus de Milo’s arms might be doing Bernard Dalens, a gent who may or may not have eaten a few snails in his lifetime, was doing some writing. Well not just Dalens but Vannueville and Tanguy as well.
Luckily for clinicians, Dalens was writing up a technique. This technique was a new variant on an old trick – put a needle in once near the groin and block three nerves.
This crew were keen on local anaesthesia applied to peripheral nerves. Keen enough to work away at making the 3-in-1 block described by Winnie work. They weren’t entirely impressed though. Although the aim was to produce block of the femoral nerve, lateral cutaneous nerve of the thigh and the obturator nerve, they weren’t happy with the bang for buck. Plus, at that stage, they were relying on paraesthesia to figure out where to put the magic mix. (This alone gives some context. No nerve stimulators. Ultrasounds are deployed more often by echolocating dolphins than medical types…) Kids struggle to describe paraesthesia accurately enough so the technique was tough. Honestly why do 3 year olds make you do all the work?
So they went back to the anatomy and defined the space. The femoral, lateral cutaneous, genitofemoral and obturator nerves all run for at least a bit behind the fascia iliaca. As it turns out the genitofemoral nerve also spends a bit of time in the area though you rarely seem to see that mentioned in modern chat.
The team went on to study their block in 120 patients. They used 0.7 mL/kg in kids under 20 kg then somewhere in the region of 0.5 mL/kg of their local anaesthetic solution (they actually mixed some 1% lignocaine and 0.5% bupivacaine).
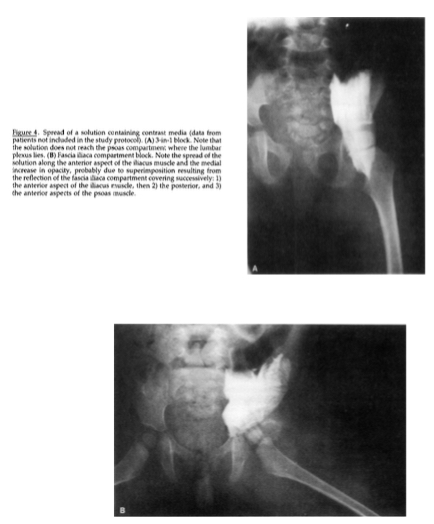
Original shots from the Dalens paper. The spread for the 3-in-1 is at the top, and the fascia iliaca is at the bottom.
More pleasingly for them I bet was that real world people responded to their plan just like the real world cadavers said they would. They had very good results for femoral nerve territory sensory blockade, but also obturator and lateral femoral cutaneous nerve areas. They also tended to have less motor deficit than the ‘find that femoral nerve technique’.
So why isn’t everyone using it every chance they get? Well I don’t know that but I know that it should be an easy to trick to pull out of the hat where the rabbit shacks up. So here’s the quick review that will hopefully inspire you to break out a needle to sort that pain…
When would you do it?
When wouldn’t you really? Any time you might consider a femoral nerve block it’s worth considering the fascia iliaca block. For anaesthetic purposes, any operations where the femur itself is going to be messed with, or the hip operations where you can add to that the distribution of the lateral cutaneous nerve of the thigh. What might be less obvious is that knee operations may also be associated with less pain if you deploy one of these, even though you’d think the sciatic would have a bit to say there.
The benefits in dealing with thigh bone pain are also just as evident with fractures. There are plenty of papers from the kids’ emergency department battle realm suggesting superior analgesia with fascia iliaca blockade compared to systemic analgesics. You can take it from me that benefit extends all the way to the roadside when an accident occurs. These are one of the few useful blocks when you’re doing work on the road. That’s medical care on the road type work. Probably don’t just needle random people on the street.
Using Sound
There are some people out there who are very passionate about ultrasound. They’ll try to add sound-based eyes wherever they can and this block is no different. Blaine Miller described an in-line technique where you locate the vascular bundle in cross-section then rotate into a view in the sagittal plane while keeping well orientated enough to know where the fascia iliaca. You also slide laterally to keep away from the big things full of blood. The needle as it lines up with the probe heads in a cephalad direction.
Others describe a long-axis use of the needle but the visualization of the vessels remains in the short axis. There’s a good example of that description on the NYSORA website (and the whole description of the block there is worth a close look). I can’t do any better than the images and descriptions of where you should put the local anaesthetic that they’ve got there. Such pretty pictures.
The bigger question is whether the ultrasound is worth it. To date there isn’t good evidence that ultrasound enhances safety, particularly with a block like this where the landmarks technique keeps you well away from vessels then you just add lots of volume. You’re not trying to give the smallest amount of local anaesthetic possible as close to the nerve as possible. You want distance from the nerve with your needle and volume to get it there.
So if you’re not going to localise it close to the nerve, your success rate is unlikely to go up (and the clinical technique is close to 100% at least for the femoral nerve) and your safety profile is the same, then what does the ultrasound add? Oh, that’s right. Time. A delay to analgesia.

Dolphins: echolocating and flying for as long as we’ve known.
You can make an argument for ultrasound that is more forgiving of these factors. It’s certainly a good block for improving your skills with ultrasound needle guidance. But if we’re talking about the emergency department I’m not quite sure why you’d use a technique that’s slower to give a kid pain relief.
Using Topography
The landmarks technique is pretty straightforward if that’s your preference. Draw a line (in your head or on the patient) between the ASIS and the pubic tubercle. This line is the inguinal ligament. Divide it into thirds. At the point where the inner two thirds of this line joins up with the outer third, step down towards the feet a couple of centimetres. You’ve found your entry spot. As a quick double check, you should feel the femoral artery pulse a few centimetres medially. Now you know which way not to point the needle. As an extra point, actually marking the location of your entry site and the artery isn’t a bad idea. It’s worth being orientated the whole way.
Little Tips
There are some little tips that just might make it easier. These aren’t the “have everything ready” type of tips and I’m going to assume some basic things will be in place (monitoring for example). This is just some of the practical stuff along the way (with plenty of scope for others to volunteer their best bits):
- Numb the skin
If the patient is awake, life is a little easier if you’ve added local anaesthetic to the skin.
- Make a hole
The technique relies on a double “pop” sensation as the needle advances through fascia lata then fascia iliaca. Sometimes the first of these pops is pretty close to the skin and if you’re a little heavy on the use of your muscles, you can pop straight through in trying to make it through the skin. So consider making a hole with something just a little bigger than the needle you’re planning to use for the block. That way, when you start advancing your block needle, you won’t be fooled by the body’s biggest organ. Pesky old skin.
- Use the right needle
There’s a distinct advantage to using the right sort of needle. Assuming you’re doing the landmark technique, a short bevel is essential. It’s the bevel that gives you the two pops. Sharper needles give you very little feel. If you’re using the ultrasound, then it makes sense to use a needle designed for ultrasound if you can. The pops aren’t so important there because you’ll be using what you see to choose the final needle position. A needle that lights up better makes a whole lot of sense.
- The advance
It’s very important with the landmark technique to make sure that needle doesn’t head towards the artery. Keep it straight up and down the line of the body (or the line of the sagittal plane). Obviously if you’re deploying the ultrasound, you watch the needle and judge it that way.
When advancing the needle, steady forward pressure is key. When you pop through the first layer, I’ve always found it useful to pause for a second and let things settle. I then do a second steady advance to achieve the second pop without any doubt in my mind that it’s definitely the second fascial layer I’ve breached.
- The mix
I’ve heard a bunch of different cocktails over time. Dalens and crew mixed long- and short-acting agents. I tend to do that in prehospital medicine because every minute waiting for stuff to kick in is a minute too long. The short-acting agent is an attempt to get an extra bit of time in that patient’s day but it’s not really the setting to trial different mixes and see how much variance there is. In the hospital though, it might be simpler for everyone to agree on a suitable long-acting agent and dose accordingly. Any of the longer-acting local anaesthetics seem like a fair choice.
I do tend to add clonidine to peripheral blocks (as mentioned here) as an adjunct aiming to increase block duration, as long as there aren’t particular contraindications to that strange beast of a drug.
- The volume
Volume matters here because that’s what provides the spread. Once you’ve figured out what the maximum dose of local anaesthetic to safely use might be, it’s easy enough to dilute with some normal saline to get to those thresholds. While Dalens and crew might have described ranges of 0.5-0.7mL/kg there is a number that’s easier to do maths with than 0.7. That number is 1.
1 mL/kg provides good spread and easy maths. The fascia is attached all the way up at the vertebral colum and upper part of the sacrum. It covers all across the psoas muscle. This is a big space. There’s not much in the literature I could find that talks of volumes anywhere beyond 40 mL though so that’s probably an effective upper limit.
Notes of Caution
I’m not going to mention a whole lot about local anaesthetic toxicity here. That’s it’s own topic and no one should be embarking on a block without monitoring in place and thoughts on how they’ll diagnose it (more of a challenge in the anaesthetised) and what they’ll do.
I did find one paper which raises a topic that is worth thinking about: rehab.
A team out of the Mayo Clinic have published a cohort study where they’ve looked at kids (mostly adolescents) who have had surgery to repair an anterior cruciate ligament and split them into those who had a femoral nerve block and those who didn’t as part of their analgesic plan.
They weren’t interested in the pain so much. Well, I’m sure they care about that stuff but that wasn’t so much the point of the study. They were interested in the rehab.
The point of that surgery is restoration of dynamic knee stability and a return to the sorts of activities that led to the injury. All the patients went through a “comprehensive rehabilitation program”.
What they found was that at 6 months, more of the kids in the femoral nerve block group had a deficit in particular parameters of strength. The functional tests weren’t so much different but the patients in the control group were cleared to return to sport earlier.
So what do you make of this? We are talking about femoral nerve block rather than fascia iliaca block so it’s possible there is a difference there. Tourniquet time was longer in the control group and adjustments for those factors still left the issues above. The weakness didn’t translate to deficits on dynamic testing, but return to sport was slower.
It’s one study. It has some issues with the methodology that shouldn’t make any conclusions too definitive. The numbers aren’t big and maybe deploying the local anaesthetic in a way where you try to get close to the nerve would make a difference but it should raise nagging questions. It certainly wouldn’t be enough to make you shy away from this technique, but it is a reminder that long-term stuff that impacts the rest of patients lives should be front of mind for acute care medical types.
It probably also means those doing the block should try to keep an eye out for the orthopaedics and sports medicine literature, just in case these sorts of findings are an outlier. Ugh, I just shuddered a bit at the thought of reading ortho journals but I guess you have to do what you have to do.
So there it is. The fascia iliaca block: established 1989 and only getting more relevant. There are still different descriptions on how to do it (landmark vs ultrasound, different probe orientations …) but the minor variations aren’t the key thing to worry about, as long as the technique is safe.
I’m more interested in the variability that isn’t so acceptable: the bit that stops people doing this five minute procedure. What are we all waiting for?
Reading:
That original Dalens paper is this one:
The case report describing ultrasound use by Blaine Miller is this one:
After a bit on the benefits of using fascia iliaca block in paediatric femoral fractures? Try here:
And for a review on whether ultrasound makes blocks safer, here’s this (from 2009 but still):
Oh, and that sports medicine paper is this one:
And here’s an interesting letter in response.
That image of dolphins is in flickr Creative Commons and is unchanged from the post by r3dc3ll

Good stuff as always Andrew. Regarding ultrasound and vessels there are sometimes small perforating vessels passing through this plane. If you throw the colour on and look for them you can often find something (and then avoid). Urban legend tells us about some poor Victorian anaesthetist who managed to get a haematoma causing a femoral neuropraxia from one of these (adult world) presumably from hitting one of these vessels
Donald
LikeLike
Thanks Don. This is a very good point and is perhaps an extra one in the ‘pro’ column when it comes to ultrasound.
LikeLike