
This post is pretty much a talk given as part of the airway workshop at the Paediatric Anaesthetic Congress of South Africa, 2019 in Johannesburg by Andrew Weatherall. A 10 minute blast through what’s actually difficult.
Sometimes we need to just take a deep breath. A pause. A chance to look around. A chance to marvel at the fact that bootleggers in Russia who really liked music but couldn’t sell records used to make records out of old X-ray film. And that is a fresh look at something that gets barely noticed.
Or of course we can take stock and look again at something that seems so easily part of what we do and discuss:
“What is actually difficult about kids’ airways?”
[This is a moment where I have metaphorically paused dramatically for you to mentally have a conversation with yourselves that is solely about kids’ airways and not at all likely to degenerate into a pondering of the shopping list or a random toenail in the carpet that probably has a backstory or why belly button lint is so often blue.]
Now that that’s done let’s get back to the literature to try and figure out what’s actually difficult in kids’ airways.
First up…
Is actually not just about the bit that’s difficult. Before we go anywhere let’s pause and think about all the times it is not difficult. After all that’s still the overwhelming part of the story. Before we get into the things that make us sweat we should maybe think about that.
A useful lily pad to land on here might be the APRICOT study and the snapshot it provides around airway management. A wide angle snapshot taken over 2 weeks in Europe with 31127 anaesthetics in 30874 patients. 4970 facemask anaesthetics, 13671 intubated patients, 10918 supraglottic airways and 129 tracheostomies (with a small subset of 1336 sedation only cases).
And 38 cases of reported difficult intubation (that’s 0.28% to save you the calculation though, bafflingly 120 patients required 3 or more attempts at intubation and don’t seem to be in that 38), a 99.5% success rate with supraglottic insertion and zero can’t intubate/can’t oxygenate scenarios.
So while we won’t to focus on the things that are difficult to get better at them, let’s not lose sight of how overwhelmingly OK things are most of the time.
And now to the horror.
The Fearsome Four
Alright, not horror. There are maybe 4 areas to really look at.
- The patients.
- The techniques.
- The place.
- The people.
- The Patients
There are a few obvious standout features and they probably match with what your gut would say. At least when it’s not dealing with hunger pangs.
In the APRICOT study, amongst the kids who were difficult to intubate the risk was higher in neonates and the under 1s. SGA insertion was also more often a problem in neonates. In the big version of the PeDI airway registry, where they are looking at definite difficult cases, kids under 10 kg had more intubations (and complications). Kids with a short thyromental distance also fell into that group.
And NAP4? Well there were 10 kids with reported complications and 9 were under the age of 4.
So small kids are tricky.
What about specific findings in the patients rather than demographics? Well Sheeran et al have a quite good report on the patients in the difficult airway registry they set up after events in their hospital.

When you look through the risk of patients with airway obstruction it’s really obvious that it starts from the top end and goes down the airway.It’s jaw, neck, TMJ, tongue before anything else even comes into it.
Oh, another quick note on the way past – of their 164 difficult intubations, only 3 were unanticipated. Assessment is useful maybe.
What about specific syndromes? Well I’ll level with you. I really struggle with remembering what each syndrome means. But here’s the list they included in that paper.
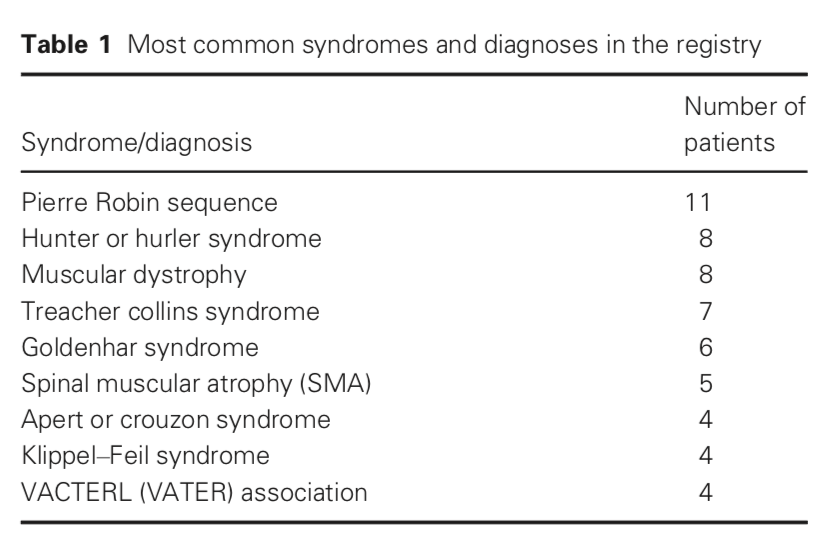
What I would say is that even without remembering that Pierre Robin is the small jaw one, or mucopolysaccharidoses result in lots of deposition, these conditions should be fairly easy to spot as ‘there is something to pay attention to with the airway’. In particular a look from the side as well the front to check the size of that jaw will help a lot.
- Techniques
Unsurprisingly face-mask ventilation gets a little lost when people go doing studies, maybe because it’s so much harder to measure what ‘good’ and ‘bad’ look like or describe techniques in a useful or reliable fashion.
Valois-Gomez et al have previously indicated that in an unselected Montreal population the difficult face-mask ventilation rate was 6.6%. They did however include using CPAP of anything more than 5 cmH2O as difficult and a lot of people would just call that ‘technique’.
What is clear in the difficult airways that look at this technique is that while there can be associated difficulties with face-mask ventilation, complete inability to do so is rare. In the PeDI papers for example, of the 821 patients with an anticipated difficult airway, 67 were difficult (that is a whopping 8%) but only 5 proved impossible to do so. Interestingly there was no attempt at face-mask ventilation in 95 patients.
In the anticipated difficult airway group there were only 10 cases where face-mask ventilation was rated as difficult (about 5%) and a single case where it was impossible. Overall in 1018 cases, there were 77 cases were face-mask ventilation was difficult (7.6%) and 6 total cases where it was impossible.
This is a technique to rely on.
Supraglottics aren’t so well covered in PeDI because in 810 of the 1018 cases there was no attempt at one. Perhaps that 99.5% success rate in APRICOT is the most informative number here.
And intubation? Well again APRICOT suggests they go well most of the time. The main thing to note is that when we have a truly difficult airway, videolaryngoscopy is overwhelmingly more likely to result in success (both on the first and subsequent attempts).
- Location
Often the consideration of difficult kind of stops there. But we manage patients in actual places under actual clinical conditions so the place we look after them should come in for consideration.
Anaesthetists are used to looking after the airway in theatres but there are tigers beyond the doors. One example is highlighted nicely by the paper by Long and Sabato which describes a year’s experience in the busy tertiary paediatric ED at Royal Children’s Hospital Melbourne (they see over 80000 patients a year).
In total there were 71 intubations in the ED in the year they sampled. 39% of them had a complication. Now things like frequency of exposure are a part of that but it is definintely the case that patients in the ED who need to be intubated are probably in the *not well* group.
The ward is no friendlier. Bai et al looked at 132 intubations by paeds anaesthetists outside theatres including the wards (but also ED) – the difficult intubation rate was 10.6%. Not quite APRICOT.
11 of 14 needed something other than direct laryngoscopy and the major adverse event rate was 3.8%.
Locations should confront us.
- The Team
Team experience probably counts once things are difficult. In APRICOT there wasn’t an obvious difference with seniority, but in the PeDI paper mentioned here, 21% of first attemps were by consultants but once you look at who eventually had success, 41% of the time it was the consultant.
The Rare Things
Hen’s teeth. Hen’s teeth are rare.
Also front of neck access. 0 in APRICOT and only 19 in the whole PeDI registry of definitely difficult airways (or 2%). Obviously we should know what we’ll do but it’s fair to say ina world where supraglottic techniques mostly work, we have options.
One Oher Thing
The corollary of this is that we should make our assessment take into account all of the factors around airway management. Not just history/exam/investigation but the patient’s underlying conditions, their acute illnesses that might change how things stand, the clinical scenario we’re in (the place the patient is, the time of day, the urgency to get on with things) and the strengths and potential weaknesses of the team. After all, airway management is a team sport.
A mnemonic like PAST might be more useful for real world use…
Patient
Acute changes
Scenario
Team
The Key Bits
So after all that looking afresh reinforces some simple things we knew. Mostly it’s simple. Sometimes it’s not. Supraglottic techniques work.
And Russian bootleggers spin X-ray vinyl.
Wait, that bit is new.
The References:
The APRICOT study is this one:
That PeDI paper (one of many) is this one:
Fiadjoe JE, Nishisaki A, Jagannathan N, et al. Airway management complications in children with difficult tracheal intubation from the Pediatric Difficult Intubation (PeDI) registry: a prospective cohort analysis. Lancet Respir Med. 2016;4:37-48.
And Sheeran’s airway registry paper is this one:
The Valois-Gómez face-mask one is this one:
That ED paper is this one:
And the one that includes wards…
Bai W, Golmirzaie K, Burke C, Van Veen T, Christensen R, Voepel-Lewis T, et al. Evaluation of emergency pediatric tracheal intubation by pediatric anesthesiologists on inpatient units and the emergency department. Pediatr Anesth. 2016;26:384–91.
