
Not that long ago, Dr Andrew Weatherall had the job of facilitating a discussion about neonatal anaesthesia at the annual Society of Paediatric Anaesthetists of New Zealand and Australia conference. About 15 people were there and this is a best effort at trying to collate the things those clever people said.
Let’s start with the tiny patient.
Today’s patient is a 2 week old boy, weighing in at 4 kg. They were born at term after an uneventful pregnancy. After birth he had a brief period where he needed some oxygen but he made it to the ward within a few hours and was home at around the time you’d expect. Beyond the intense adjustment that comes with having a kid at home, the first week or so had been pretty unremarkable.
Until one day when the kid seemed to have some sort of coughing or choking episode around the time of a feed and seemed to maybe go a bit floppy. Or at least different in a way that worried Mum.
So he arrived at his local hospital where they noticed he was breathing pretty fast, although his saturations were surprisingly normal. They started a bit of oxygen hoping it would help the work of breathing they were seeing. And they did a chest X-ray.
That was enough to make them get going with antibiotics. Things didn’t change though so they decided to transfer the kid across to the big hospital.
Now, here’s the X-ray the kid initially had…..
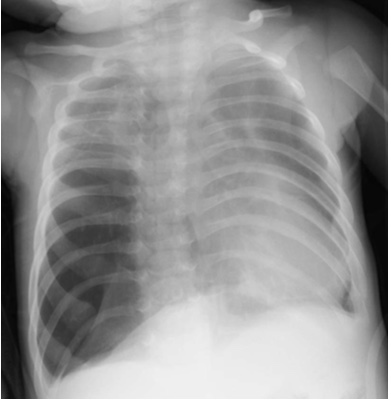
I don’t know, there’s just something about it that makes me think it’s not normal …
What do you think? Where is the pathology? Right or left?
(Now, I actually want you to ponder that so I want some separation before the next photo …
so I’m going to put some random stuff in here….
to pad ….
like…
Did you know that in the movie version of ‘Fargo’ there’s an actor who plays a person who gets shot in the snow and it looks like their credit at the end is the symbol Prince used when he was in that contract argument with Warner? So people think it’s Prince making an obscure cameo (but last time I checked it’s not)?
OK is that enough thinking time on the X-ray?
Because the respiratory team now see this patient working hard, notice a couple of extra clinical signs and think a CT is worth it. (Now I’m not going to go into the details of how to anaesthetize for the CT because we’re moving along, but for general principles that you could start with then adjust see this post.)
The patient gets their CT.

Whoa, right?
So now the patient has their diagnosis and it’s congenital lobar emphysema. You can really see on the CT how that right middle lobe is pretty much everywhere and probably not superb at doing the job of normal lung. The kid is getting by on not much left lung and not much of the other bits of the right lung.
Congenital lobar emphysema is not a pleasant beast to deal with, and while it’s a bit beyond the scope of this little post to go into the details, it is worth knowing that the commonest cause is some form of bronchial cartilage dysplasia or deficiency leading to a segment of bronchomalacia. Air trapping can be the result and this particular kid has exactly that picture.
Of course, the surgeon wants to get it out this afternoon.
[Now, a sidenote here. When I presented this in the PBL session I made the timing a little later and a bunch of people attending indicated that they would have pushed back very hard and suggested that a kid who had been chugging along for a couple of weeks would probably be fine to wait until the morning to optimise the time of day. I think all of those who said this made a really good point. What I can also say is that in the case this is based on, the surgeons and respiratory team became most insistent once they’d seen the scan that they weren’t comfortable waiting any longer and the kid was starting to look like they were working harder. We could have done a whole PBL on the interaction between your prior experience, the characteristics of the individual clinicians and the effect of seeing a scan on your clinical assessment of where the patient is at, but of course it was a PBL and we had to get on with the imaginary case.]
So what are the challenges of this case?
On throwing this one to the room there were a couple of things that came up quicker than you might have thought. The conversation didn’t entirely just come down to “keep them warm, wet, pink and sweet”. The hot topics for discussion were:
- What IV access do you want?
Consensus in the room was in this patient a couple of reliable peripheral IVCs would be adequate. This was partly coloured by a desire not to delay the crucial surgical bit while gaining central access. If the kid had a cardiac history a couple of people indicated this might shift their thinking.
- What tips do you have for getting that peripheral cannula in?
There were a few top tips here, but it turns out nothing that hasn’t popped up in a post on this site before right here.
- Arterial cannulation?
Yes. Everyone said yes for this. There are some cases where you don’t work so hard to get that arterial line if it doesn’t work out easily. Everyone really wanted one for this sort of case. (We also recently posted a collection of thoughts relating to doing them clinically here.)
- Which fluids?
The majority in the room would leave some maintenance going continuously to ensure adequate glucose throughout, with boluses as required. The most frequently quoted sugar rating on the bag? It seemed to settle in at 5% glucose as part of the mix, though the key message was that there should be some glucose and there should be regular reassessment.
There was a mix in the room between those who would want cross-matched blood in their theatre complex or not. As it turned out this mostly came down to how quickly they’d expect a unit to turn up when they called for it. Any more than 5-10 minutes and people thought it was worth having it right on hand.
- How do you approach ventilation where there is a risk of air trapping?
Now it turns out there is nothing in the way of evidence to tell you what pressure works. The consensus in the literature is that you should try to avoid peak pressures above 20-25 cmH2O and excessive PEEP but it’s pretty obvious that amounts to a “we reckon” level of evidence. You can also find reports of kids who have been chugging away on ventilation for a prolonged period of time before the diagnosis. You can find reports of management of these kids with HFOV. No one can really define what critical pressure will lead to expansion of that emphysematous lobe. Everyone in the room said they would use a high FiO2 to maintain oxygenation and everyone agreed that a degree of hypercarbia was to be expected.
There was a mix of opinions on whether individuals would feel most comfortable maintaining spontaneous ventilation until the lobe was delivered vs whether they’d control the ventilation (most who went down this road seemed to feel that spontaneous ventilation would be hard to maintain and if you then felt the need to manually ventilate you might be more likely to be overenthusiastic with the bag in hand). Again, a diversity of opinions sort of suggests there’s no perfect answer.
6. Would you isolate things?
Lung isolation ended up a hot topic as one way of guaranteeing you don’t inflate that lobe is to ventilate only the other lung. But wait, could you get by just ventilating that left side? Well if you go back and look at that CT you’ll probably reach the same conclusion as a few in the room – the patient is already getting by on those collapsed slabs of lung usually known as the left upper and lower lobes.
As to isolation options (assuming you were even going to try), well some would just go with an endobronchial intubation, while there was a little discussion about using bronchial blockers in all their fiddly overly mobile glory.
A couple of tips and tricks from the room on this one:
- If you’re trying to get the tube down that right bronchus, you can rotate the head left as you advance and rotate the tube around 900 to the right. Or of course ask a student to intubate and deploy their enthusiastic over-insertion.
- If you’re aiming for the left side, turn the head right and rotate that tube even a bit beyond 900 anticlockwise as the left main bronchus tends to head a bit more posteriorly.
- Or of course you could use a bronchoscope and actually see things.
And if it comes to bronchial blockers you’ll place it outside the tube and try to get it in that right bronchus. Let’s just assume that once you place it all will be good and not prone to needing repositioning. Hey, we all have dreams.
Now the technique I’ve used on the handful of times I’ve deployed a blocker is to put a small kink in the blocker (as described here) and deploy that slight bend at the end to help guide it into place (under bronchoscopic vision). Another option was described at the meeting in another session which involved deliberately endobronchially intubating the side you want to end up with a blocker and then putting the bronchial blocker inside the tube and pushing it into the bronchus. You then pull out that tube leaving the blocker behind (the tube ends up just hanging outside the mouth next to the head. You can then bag (back to the facemask) the patient a little to oxygenate and put your tracheal ETT in followed by flexible bronchoscopy via the ETT to place the blocker.
I have to say that this seems a lot more complex than just “put the blocker in, put the tube in, place the blocker with the scope” which is the version I’ve done before. I also figure that in this case with CLE you wouldn’t even want to add one breath when you’ve got that initial tube down the bronchus to the dodgy bit of lung. So I can’t say I saw any advantage to this option. People say it works though.
How do you get a look in?
One of the big challenges with neonates is being able to keep the metaphorical eyes on them. Now a couple of attendees indicated that their hospitals use see through drapes so you can keep eyes on the patient and I will absolutely be tracking those down. A lot of the time you end up using monitors to feed back the vital information that tells you where you’re up to. So the next topic for discussion was “which monitors and what do you do with them?
- Pulse oximetry.
The obvious first cab off the rank which everyone reached for was pulse oximetry. You get a little information about oxygen and a little information about distal perfusion. Everyone in the room opted for two in this case, partly to protect against the interference provided by a leaning surgeon, but also to offer pre- and post-ductal saturations just on the off chance that some transitioning to a not-so-series circulation happens.
One good word of warning that emerged in the discussion is that a lot of the modern pulse oximeters auto-scale to make the trace look good. This looks pretty on the screen but it can give you the impression that the distal perfusion is good when it is like a distant echo of rushing blood or that you can rely on the number it’s spitting out when neither is true.
- End-tidal carbon dioxide.
In a case where ventilation is crucial and a bit at a risk of being threatened and where a ball-valve situation is a real risk with ensuing haemodynamic compromise could happen this is clearly an important one.
- ECG
Unsurprisingly this was also considered to be vital, not so much because of a particularly high risk of arrhythmia or ischaemia, but because even when your peripheral monitors are not helping for whatever reason you have something linking you to the cardiovascular system.
- Blood pressure
As mentioned above everyone was keen on invasive blood pressure monitoring rather than just the squeezy arm version. The question is what BP are you happy with? The classical teaching of “aim for a mean pressure around gestational age” doesn’t seem to have much to back it up. It’d be nice to have something better.
Well a few papers have come out recently that might provide slightly firmer numbers to work off. A paper by Sottas looking back through electronic records gives some sense of the normal range of falls in blood pressure. The suggestion was that there was fall in the region of 16-30% in kids under 10 weeks old around the induction of anaesthesia (for MAP they quote 16.6-34.5% and systolic 16.3-32.6% fall) was expected. There’s some additional stuff from a big retrospective cohort study from de Graaf and friends suggesting the 50th centile for mean arterial pressure at birth is 33 mmHg.
That’s great but what about functional evidence? Well Michelet and crew published a paper not that long ago looking at cerebral tissue oximetry (the non-invasive kind) values across 69 patients under 3 months old. They found that if the non-invasive blood pressure fell less than 20% from baseline there was a < 10% chance that you’d see evidence of cerebral desaturation.
Rhondali and team have also published some stuff in this area, sometimes looking at cerebral saturations and sometimes at cerebral blood flow. They were tending to see a fall in blood pressures around induction (with sevoflurane) of around 30% from baseline. In the cerebral blood flow study they suggested flow dropped once MAP fell below 38 mmHg (or a fall of 20% of baseline) in the under 6 month kids. When it came to regional oxygen saturations, things looked OK for as long as MAP was above 33 mmHg (in patients under 6 months old).
So it seems like there’s some evidence to support really knowing your baseline blood pressure (which may be best achieved by looking right back through observations taken prior to theatre) and then keeping it within 20% of that (or above an absolute value of 35 mmHg). Sounds pretty sensible.
- What about NIRS?
Well NIRS (that is near-infrared spectroscopy as a technique to provide measurements of tissue oxygenation) is still trying to find its place in the world. This post is waaaaay too long to also include a review of all things to do with shining lights, but I did have a trace from a similar thoracic anaesthesia case to work through.
So take a look at this trace where peripheral saturation is shown in blue, regional saturation (the NIRS value) is in green (and pretty solidly initially in a pretty standard 60-80 range) and invasive blood pressure appears in red.

Now a couple of things you might note here:
- See that big upsurge at the start of the case in the rSO2 (the regional saturation)? This is sort of an “anaesthetic margin” which seems to come with the initial drop in cerebral metabolism/delivery of plenty of oxygen/control of carbon dioxide.
- If you haven’t used NIRS oximetry before you can really see that the monitoring response is quick.
- Before the red blood pressure line kicks in you can see a cerebral desaturation that mirrors a fall in saturations. In this particular case this was around the time of repositioning onto the side, and represents a disconnection.
- You can also see a distinct rise in blood pressure (between the 2 and 2.5 marks on the x-axis) which is at incision, but there is then a fall in blood pressure, followed by cerebral saturation just before peripheral oximetry values fall.
This last one suggests a primary change in haemodynamics led the change in cerebral saturation (a momentary Valsalva might be one explanation).
So what NIRS can potentially offer is corroboration for when an alteration in oxygenation or haemodynamics is something that matters to the end organ. It can also probably indicate which is the primary problem (blood pressure first vs oxygenation first) though you’d have to be very attentive to pick it up in sequence and it’s more likely to be useful in deconstructing things later. It’s also worth noting that overlapping the traces like this isn’t something the clinician would readily have available with a commercial monitor just added into their system. It does demonstrate where it might all be heading though.
Now NIRS discussions could go on for a long time (feel free to hop into the comments and we can do just that) but I think this PBL could probably do with wrapping up (well, this written version of it anyway).
So you set things up well. You have the access you wanted, the monitors you like and the patient has good plans happening with analgesia and fluids. Then there is a fall in BP, ventilation gets harder and everything gets very urgent as the saturations fall.
And the surgeons finally (and rapidly) get the crucial bit done and deliver …

… a lobe.
And after that it’s just pink, warm, wet and sweet to bring it home. Plus some good analgesia. (OK, there’s a little more to it than that.)
This is just an attempt to capture some of the discussion in a PBL about neonatal anaesthesia. The aim was to reflect some of the things that a group of people in a room thought mattered a whole lot. It is absolutely not the whole answer to all of neonatal anaesthesia but I threw in as many points as I could remember to squeeze in. Plus a little bit about Fargo that’ll work out for your next trivia night.
Notes:
The case used in the PBL is an amalgam of a couple of cases. The main part of the case comes from the publication I’m about to list and the NIRS readings come from a separate case for which permission was also granted to look at traces (but I’ve provided no identifying info). Here’s that paper:
Here’s that paper on endobronchial blocker techniques again:
And now the BP papers:
If you’re after a pretty good general summary of NIRS in kids anaesthesia, try this one:
An acknowledgment also to Dr Justin Skowno who helped out a bit making sure I had some good references around the BP and NIRS stuff.
This of course is just an effort to share thoughts from a discussion. It is by no means a complete thing and we’d love to hear comments or thoughts from far and wide so go ahead and comment away.
And if you think the site is OK don’t forget you can follow (look around the page, it’s here somewhere) and you’ll get an update when a new post hits.
Finally, did you scroll all this way? You are a true hero. You should reward yourself by watching this truly excellent day out on a mountain bike with Danny McCaskill. It’s worth watching to the end too.

Pingback: What Will You Do With This Tiny Person? — Songs or Stories | Prehospital and Retrieval Medicine - THE PHARM dedicated to the memory of Dr John Hinds·