
This is a slightly different bit of sharing. Dr Andrew Weatherall works at The Children’s Hospital at Westmead where they’ve been quietly working away at a redesign of the difficult airway trolley. Here is the story so far …
Middle age is not always kind. You start to look a little tired. Nostril hairs are a thing. And grey hairs. Actually hairs feature more than you’d think. I am told. By other people. All the other people. *Cough*
This is something that applies not just to people (other people, remember). Sometimes the way we go about our work carries just that little bit of extra flab or the stuff we use has just accrued a slightly untidy air about it.
Which brings us to the airway trolley we’ve been using in my neck of the woods. Which … well, needs a facelift honestly.
How did we get here?
I am lucky enough to work with a heap of extremely clever people. They do extremely clever things. That includes managing really tricky kids’ airways and developing a heap of skills over a pretty long time.
Along the way people surely developed a trolley to retain our bronchoscope gear and a few tools for difficult airways. And then some people probably added a few other things that you might need. And a few other things you might need. And that one thing that one person really likes.
So where does that lead you? Well, maybe around about here.

Sorry, did you want some kind of airway introducer? They’d be here…

Yep, that’s around the back somewhere.
And look, the stuff is there and clever clinicians make it work. But it’s sort of a hulking mess of stress and regret. We had really got to the point where we felt it just wasn’t user friendly enough and didn’t make it easy to get on with the job. And when time pressure was a bit of a factor this trolley runs the risk of making things harder, not easier.
Once other items like video laryngoscopes became available the use of various airway devices was getting more fragmented. Not such a drama for planned difficult airways, which is the overwhelming majority in kids’ anaesthesia. Start making me imagine those sats falling and a request for urgent stuff though and … well I didn’t know you could sweat through your fingertips onto the keyboard but this is a place for learning.
Time to Reset
So the first hurdle was cleared. A bunch of us wanted to tackle a redesign but the question was where to start?
We do not come with backgrounds in design, or engineering or anything much but kids’ anaesthesia really. So what follows is a pretty haphazard description of how we thought about things and where we have got to so far. It’s not perfect, and it is absolutely a work in progress that will need constant revision and tweaking. But here it is, for passing bowerbirds to pick over and pick apart.
Here’s what we did and what we thought about, in technicolour detail.
1. Look far and wide
The first thing we did was look around. Plenty of our colleagues work at other places encompassing private hospitals, adult hospitals, other cities and even retrieval organisations.
The thing we noticed about plenty of airway trolleys when we checked them out in person, from publications or from shots online was that they sort of addressed a problem that we didn’t feel was a problem.
A lot of the trolleys seemed like they were designed for the planned difficult airway. This is the sort of airway where you have the luxury of time to casually sift through an endotracheal tube plantation for the exact thing you want, and move from drawer to drawer to grab that one little widget.
Even where there was plenty of order to the contents, we kept seeing tight-packed drawers with everything we could possibly want, jostling like passengers in the train in peak hour.
And we decided that wasn’t what we were after. Which brings us to the key change in our thinking.
2. Figuring out our priorities
Having a multitude of options when we had time on our side was not really a good way to deal with the hypothetical situation that worried us. We were worried about that rarer occasion where we find ourselves in a tight spot where the airway is trickier to manage than we thought.
Under those conditions, too many choices become an obstacle. When we’re in a real crisis we want to have every possible part of brain space available to focus on doing the thing that needs to be done, and just as importantly, communicating to the team.
So we decided to abandon designing for every possibility. We decided to change the design question and start asking “how do we make it easier for ourselves when it’s all going wrong?”
And in answering that we started making decisions to group things in ways that helped the clinician achieve a goal, rather than grouping things on the basis of their definition (tubes must go with tubes, masks must go with masks).
3. Design with the whole team
We don’t work as solo operators. Lucky anaesthetists at our joint get to work with exceptional nurses. They invariably have clever ideas that don’t even occur to us and they are mostly way better at intuiting practical things.
So every step of the way we’ve done this as a team and bounced ideas back and forth to make sure they work for everyone who will help manage that paediatric airway.
I cannot stress how worthwhile this bit is.
4. What are the worst bits?
Plenty of us also remembered that one of the trickiest things in kids’ airways is just the amount of gear. Sometimes tiny, tiny gear but lots of gear.
One challenge in kids over adults is the range of equipment and trying to get the right size. Not just the right size for the right patient, but the right size of this equipment to go with that equipment over there.
We all had memories of fumbling under stress because we’d grabbed the wrong suction catheter, or the endotracheal tube didn’t fit down the supraglottic airway, or we’d forgotten one key bit of stuff.
Nobody has time for that stress, particularly when the sats tone is descending down somewhere in the realm of whale hearing.
So we decided we wanted:
- A trolley that made some of the choices for you.
- A trolley that helped streamline your thoughts in a tight spot.
And that needed something different…

I mean, so pretty…
The Other Bit of Looking Around
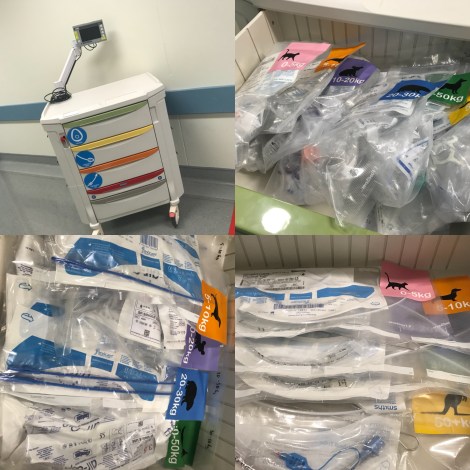
One of the things we did really like in our looking around was the Vortex approach. Much championed by the very generous Nicholas Chrimes, the resolution of the techniques available to mask/supraglottic/ETT/CICO (though the last one is very rare in our setting) had already set out much of the simplicity we were after.
So we absolutely unashamedly adopted a drawer layout to support that sort of thinking. Drawer 1 – things to optimise face-mask ventilation. Drawer 2 – things to optimise supraglottic airway insertion. Drawer 3 – things to optimise endotracheal intubation.
But that didn’t entirely resolve the equipment sizing issue. Which brings us to the bit inside the drawers.
Getting it Together

If it is all going wrong, I promise I will not do a good job of asking for the right size oropharyngeal airway for this 12 kg child in front of me. I bet that if there was a really obvious pack which already had the stuff I needed in it though I could sensibly ask for it.
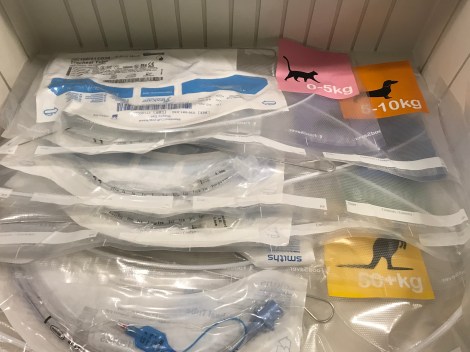
So rather than just putting all the “mask stuff” together, we decided to pack it in vacuum-sealed clear bags within weight ranges. Each bag needs a couple of masks, a couple of oropharygneals, a couple of nasopharyngeals and a suction catheter that will work. So there’s a little bit of work to get the bit of kit from inside the bag. But way less than we used to have to worry about.
“I need mask stuff for this 12 kg kid.” [Friendly helper opens drawer 1 –> grabs pack –> opens pack –> it’s all there.]
And Next…
How about we open drawer 2 with the supraglottic stuff?
This one has not just the supraglottic stuff but the tubes that will fit through those supraglottic airways, the bronchoscope attachment to help guide it, the lube and syringe you need and the pusher to hold it in place while the SGA comes out. All pre-checked to make sure that the thing fits (or fits through) the other thing.
There’s a risk people will think “well the pack has all the extra stuff so I better turn it into a tube” but if we go in knowing that we will hopefully be able to focus on training to remind people they can always pause if they are in a safe spot.
And Next?
If we go down to the endotracheal tube drawer you’ll find the bougie that matches the tube which is chosen … I think you get the idea.
The Other Features
There are a few other features we hope make this a good solution. Vacuum sealing is a little distressingly plastic-heavy, but it does guarantee you can see everything in the pack. Nothing moves. You can familiarise yourself at any time with the pack contents and it’s easy to write your up-and-coming expiry on the edge.
Feel like checking the trolley? Just check the 6 packs are there in the drawer and the upcoming use-by is OK.
Open a pack and need to restock? Grab a pre-made one from the storeroom and you’re good to go.
Oh, and did you notice there were some stickers?

These come from the creative mind of James Hutson at explanovision.com and there was a bit of to and fro.
Initially we explained the idea and said “please to give us the clever stickers that will say ‘this is the mask thing and it is for this weight range and that weight range is for this sort of kid’ and we will be happy”. James did a good version of that.
However we’d asked for a lot of detail on a small sticker. At some point someone said “the drawers already say the purpose bit so let’s just do sizes.”
Less detail allowed bolder and cleaner graphic work. The colours really hit you and the font is easy to read (even if you’re dyslexic I think). At the same time James had the very clever idea of ditching the varying small versions of humans who were a bit hard to pick apart and choose animals. Not just any animals either. Animals you can spot in profile easily, that are either Australian or companion animals (yes I have a pet wombat, what of it?) and that are in the corresponding weight range.
And the weight ranges had been chosen by us to match something already drilled into us from daily practice – weights from supraglottic airway sizing. Wherever possible we’re trying to exploit reflexes we’ve already conditioned.
Same goes with the colours. The colours are a bolder version of the colours of our usual supraglottic airway packaging. Everything we can do to short circuit the need to think is built in.
The Pointy End
Wait, I forgot the “CICO Rescue” drawer. Well it looks like this.

The cannula technique kit covers all weight ranges so it has all the stickers. There are 3 scalpel technique packs because they cover a bit of a range, so 2 stickers each. Every airway introducer is already out of its pack with any connectors already on. Each kit has a laminated card to make sure you’re working through the elements of the CICO response.
The Last Bits of Kit
Add our CMAC screen to the trolley like in the first picture (which also works with our bronchoscopes) and we’re close to good to go. The blades will fit nicely in the side bin things, and we hope to place Glidescope stuff for smaller kids in the left-side bins.
On order are some disposable bronchoscopes in the adult sizes to replace our current reusable 3.5 mm bronchoscope. Those will be attached at the back right, while our small bronchoscope for littler people and the accessories we need will go into the lowest drawer on the trolley. Everything we need and nothing more. We hope.
And The Rest
This is not at all a work that’s done. We can already see a bunch of things we need to keep working on.
1. The Education
Already in development is a suite of “ways to educate around the trolley” where we aim to have simple learning guides for anyone to run an education session from ‘let’s chat through this’ to ‘let’s open things’ to ‘let’s do a skills station’ to ‘let’s do some sort of simulation’ covering all the elements of airway care we can think of. Plus we’ll have to make sure we’re accountable for doing this regularly and refining it all the time.
2. The Kit
We fully expect to adapt what’s in the packs as we use everything more in clinical practice. That’s another part of continuing quality stuff.
3. The Usefulness Check
Yes there will be feedback. So much feedback.
4. Universal Rollout
We’re hoping to make this work across the hospital. Watch this space…
5. The Algorithm
We always assumed we’d want to have an algorithm on that top surface to act as a prompt for planned airways to encourage people to use it with all tricky airways, not just in crises. You see the thing is, when you design for the crisis situation you still end up with a pretty elegant collection of stuff for when you have time to plan. Plus we want people reaching for it plenty so it’s really familiar when they need to reach for it in a hurry.
So an algorithm that made people want to use it for the anticipated difficult airway would be perfect.
Except we’ve had a look at a bunch of algorithms and it turns out we don’t think they are really what we’re after. We have another idea and …. well, that can wait for the update.
Notes:
I may be the one writing about this but there is a big collective of people who have been part of the project. This ranges from docs and nurses who have been involved because of their enthusiasm and really put in some yards, to docs and nurses consulted regularly to chip in their extreme cleverness. I’m just the one hollering about it.
I think the Dutch hollered about it too. I’m assured they were kind.
You should absolutely check out the resources over at vortexapproach.org where the extremely supportive and generous Nicholas Chrimes has a huge amount of very useful stuff.
Did you like James’ work on those labels? You can find him at explanovision.com or on Twitter via @jameshutson
We think this will work pretty well, but it’s designed for our situation and we get that it might not suit everyone. We are super happy to get feedback of course. Likewise we’re very happy to share anything you’d like about the trolley pretty much. Just get in touch or maybe drop in a comment.
Of course if you don’t want to miss the next update, turn into a follower.
And if you like design things that influence how you do things, plus you read all the way to here, how about checking out this traffic light?

Pingback: The Airway Trolley reborn! | Prehospital and Retrieval Medicine - THE PHARM dedicated to the memory of Dr John Hinds·
Pingback: Best Laid Plans | Songs or Stories·
Pingback: The 2018 Year in Review | Songs or Stories·